Improving diagnosis in primary care one case at a time
While primary care physicians aim to diagnose patients as quickly and accurately as possible, a host of communications and record-keeping errors, cognitive biases and other factors can lead to missed, delayed and incorrect diagnosis. According to recent estimates, diagnostic errors occur in roughly five percent of primary care cases, affecting 12 million adult patients in the U.S. each year.
And while there is no easy fix, researchers and practitioners who study misdiagnosis believe changes in primary care practice and more supportive environments for clinicians are needed to improve the diagnostic safety of patients.
Compared to hospital-based peers, clinicians in primary care are less likely to have regular opportunities to examine and discuss cases where diagnostic delays or errors resulted in harm or potential harm to patients. The Primary-Care Research in Diagnosis Errors (PRIDE) Learning Network is one effort to help them learn more about diagnostic error and how to prevent it.
The Learning Network, which currently includes professionals from more than 20 organizations, brings together clinicians and others with interests in primary care diagnosis, including patient advocates, to analyze case reports in small-group discussions.
Key takeaways
The problem
Attempts to facilitate diagnostic error case discussion among primary care clinicians face technical, legal and logistical challenges.
The solution
The PRIDE Learning Network offers an opportunity to examine diagnostic error cases in small, multidisciplinary groups.
The background
PRIDE researchers have prepared cases, developed a safe legal and technical environment for discussion, revised taxonomies for diagnostic error and hosted case reviews.
The outcomes
PRIDE Learning Network observations are being shared directly with organizations, disseminated through publication and expanded through further development of the community and its scope.
Individuals from the following organizations have participated in PRIDE Learning Network discussions.
Baystate Medical Center | Best Doctors | Beth Israel Deaconess Medical Center | Betsy Lehman Center for Patient Safety | Brigham and Women’s Center for Patient Safety Research and Practice | Cambridge Health Alliance | Constellation Mutual, MMIC | Coverys | CRICO | Harvard Pilgrim Health Care Institute | Harvard T.H. Chan School of Public Health | Harvard Medical School Center for Primary Care | Institute for Healthcare Improvement | Maine Medical Center | Massachusetts Coalition for the Prevention of Medical Errors | Massachusetts General Hospital | National Institute of Justice | Northeastern University | Partners HealthCare | RTI International | Tufts Medical Center
Over the past two years, the PRIDE research team has reviewed hundreds of cases, updated taxonomy systems used to describe diagnostic errors and led discussions about a select set of cases to uncover new insights about primary care misdiagnosis. Learnings will be disseminated more broadly this year through publications in journals and on the web. Selected cases are scheduled to appear in the Agency for Healthcare Research and Quality’s WebM&M series, which reaches a large audience in the U.S. and beyond.
PRIDE is led by Gordon Schiff, M.D., Associate Director of Brigham and Women’s Center for Patient Safety Research and Practice, and is funded by the Gordon and Betty Moore Foundation. The Betsy Lehman Center co-led the PRIDE Learning Network. Most of the initial partners and network members are Massachusetts-based, but PRIDE’s founding members hope the Learning Network will become a national center that fosters diagnostic safety through the collection, study and dissemination of case reports.
Although Schiff has devoted much of the past 15 years to understanding diagnostic error, he began a recent discussion by noting how much work remains ahead: “We’re still in the early years of figuring out how to make this important patient safety issue into something where we’re really seeing traction in terms of understanding and improvement.” To gain traction, frontline providers must be able to discuss cases of diagnostic error openly and honestly, without fear of litigation.
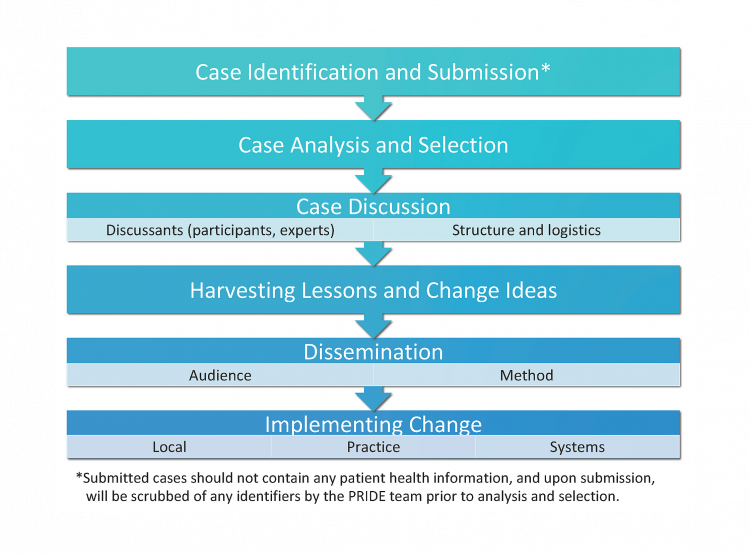
Learning about the process is key. What are the steps in the diagnostic process? What can go wrong at each phase?
A safe environment for learning from errors
Creating a safe learning environment was one of PRIDE’s early challenges. Schiff says that solving problems related to confidentiality and legal protection and finding the right health information technology host for the project were the first hurdles to overcome. Other groups have attempted to share and learn from similar cases but have not been able to get past the roadblocks.
Discussing cases where something has gone wrong — whether an error has caused harm or been caught before reaching the patient — improves understanding of possible pitfalls in the diagnostic process. Diagnosis is complex and dynamic; taxonomies created to capture the process and identify where things can go wrong are detailed and evolve to reflect current knowledge.
The PRIDE research team has been revising existing taxonomies of diagnostic error, including one first developed by Schiff nearly 20 years ago, based on the case discussions. Schiff says, “Learning about the process is key,” and encourages everyone to ask, “What are the steps in the diagnostic process? What can go wrong at each phase?”
Schiff credits Michael Cohen, R.Ph., at the Institute for Safe Medication Practices for having first applied this kind of process improvement to prescribing medications, a similarly complex process. The Learning Network encourages primary care practitioners to be process-minded as they review cases and reflect deeply as a cross-disciplinary group in a safe, non-accusatory environment. Those discussions have been more available in hospital settings, through Morbidity and Mortality conferences, for example, than in primary care.
Next steps
As they wrap up the first phase of this project, the PRIDE research team and partners are spreading lessons learned from case discussions and debating the impact of local change on a modest level compared to system change across organizations.
One of Schiff’s early visions for the project was for people to take what they learned in case discussions back to their institutions and ask, “Do we have this problem here?” Schiff models that approach at the Brigham by reviewing cases for problems that surfaced in discussion, looking for patterns that might not have been recognized before.
"Is case discussion the kind of thing we want to make sure every organization is doing within their four walls as well as across organizations? How do we get the learning into practice? And we should always remember to ask, 'Does this actually lead to improvement?'”
Although the factors that contribute to diagnostic error may appear to be “all over the map,” Don Goldman, M.D., Chief Scientific Officer Emeritus and Senior Fellow at the Institute for Healthcare Improvement, thinks that good thematic analysis would boil them down to a finite number of issues, most of which could be addressed with system change.
Others offer examples of problems revealed through case analysis and addressed on the local level with satisfying results. Doug Salvador, M.D., M.P.H., Chief Quality Officer at Baystate Health, describes an initiative designed by the hospital medicine and radiology physicians to fix a pattern of misdiagnoses by redesigning radiology reports. Salvador calls this a small change, but one that the physicians are “really proud of. It’s made clinicians' lives better and mitigates the risk of future errors. And now they’re looking to work on additional reports for similar improvements.”
Tejal Gandhi, M.D., the Institute for Healthcare Improvement’s Chief Clinical and Safety Officer, pointed to some of the challenges in this work:
"Is case discussion the kind of thing we want to make sure every organization is doing within their four walls as well as across organizations? How do we get the learning into practice? And we should always remember to ask, “Does this actually lead to improvement?”
Expanding the reach of change
Schiff acknowledges that broader changes in the way primary care is practiced will ultimately be needed. He and others in the field are working to develop pathways toward more “conservative diagnosis,” shorthand for striking the right balance between missed or delayed diagnosis and overdiagnoses that can lead to unnecessary or ineffective treatments.
Schiff looks forward to the Learning Network expanding the types of diagnoses and issues it addresses as well as the range of experts in the group, to include non-medical professionals with an interest in safety such as engineers, for example.
“Finally,” Schiff says, “we hope to increase traction by bringing lessons from these cases back to the institutions represented in the PRIDE Network so they can examine the occurrence of and ways to prevent errors that we identify in our discussions.”