Overcoming barriers to indications-based prescribing
Indications can play a role in signaling to patients that there’s a problem and stopping someone from taking a medication that’s wrong or that they’re confused about.
They are known as the “five rights” of safe medication administration: the right patient, right drug, right dose, right time, and right route. For decades, pharmacy and patient safety experts have wanted to add a sixth: right indication. They argue that printing the reason for taking the medication on the individual packaging helps prescribers and pharmacists confirm the right drug has been ordered and helps patients self-administer correctly.
Writing prescriptions has advanced greatly since the days when physicians were urged to write them in Latin to spare patients the effort of even knowing the names of their mediations, not to mention the reason for taking them. But medication processes persist as a leading source of errors and harm, and some experts believe the lack of indication is a contributing factor. Michael Cohen, R.Ph., President of the Institute for Safe Medication Practices, and Gordon Schiff, M.D., Associate Director of Brigham and Women’s Center for Patient Safety Research and Practice, are among those who have been advocating for indications-based prescribing, which involves including the indication at the order-entry phase of the process as well as at the end, with labeling.
“Indications can play a role in signaling to patients that there’s a problem and stopping someone from taking a medication that’s wrong or that they’re confused about,” says Schiff, adding it’s also helpful for pharmacists looking to counsel patients and more respectful to patients themselves. “There’s this guessing game if the pharmacist doesn’t know whether you’re taking this anti-coagulant for a blood clot in your leg or for atrial fibrillation. The pharmacists are very frustrated.”
Cohen, who began advocating for indications-based prescribing in 1975, explains, “It's good for patients to know what the purpose is. If they or the pharmacist sees that it doesn't make sense, because they don't have that diagnosis, then you could pick it up in that way.”
Despite these convincing arguments, including the indication is not the norm. In a recently published study, Schiff and others found that over a five-year period only 7.41% of more than 4.3 million prescriptions at one institution included the indication. Internal medicine prescribers generated the highest number of prescriptions, and they were the least likely to include the indication — only 6.26% of the time.
It's good for patients to know what the purpose is. If they or the pharmacist sees that it doesn't make sense, because they don't have that diagnosis, then you could pick it up in that way.
Special privacy concerns for mental health treatments or for patients with sexually transmitted diseases are among the interests that limit support for printing indications on prescription labels, but advocates say that systems can be built to accommodate such situations. Other barriers to widespread implementation include concerns about extra prescriber time and effort, limited evidence to support a change to common practice, complexities in both defining and creating indications, and creating “smart” recommendations. Most current computerized provider order-entry systems don’t facilitate indications-based prescribing.
Successful prototype may lead the way
With funding from the Agency for Healthcare Research and Quality, Schiff and his colleagues developed a prototype computer model that could make indications-based prescribing the standard.
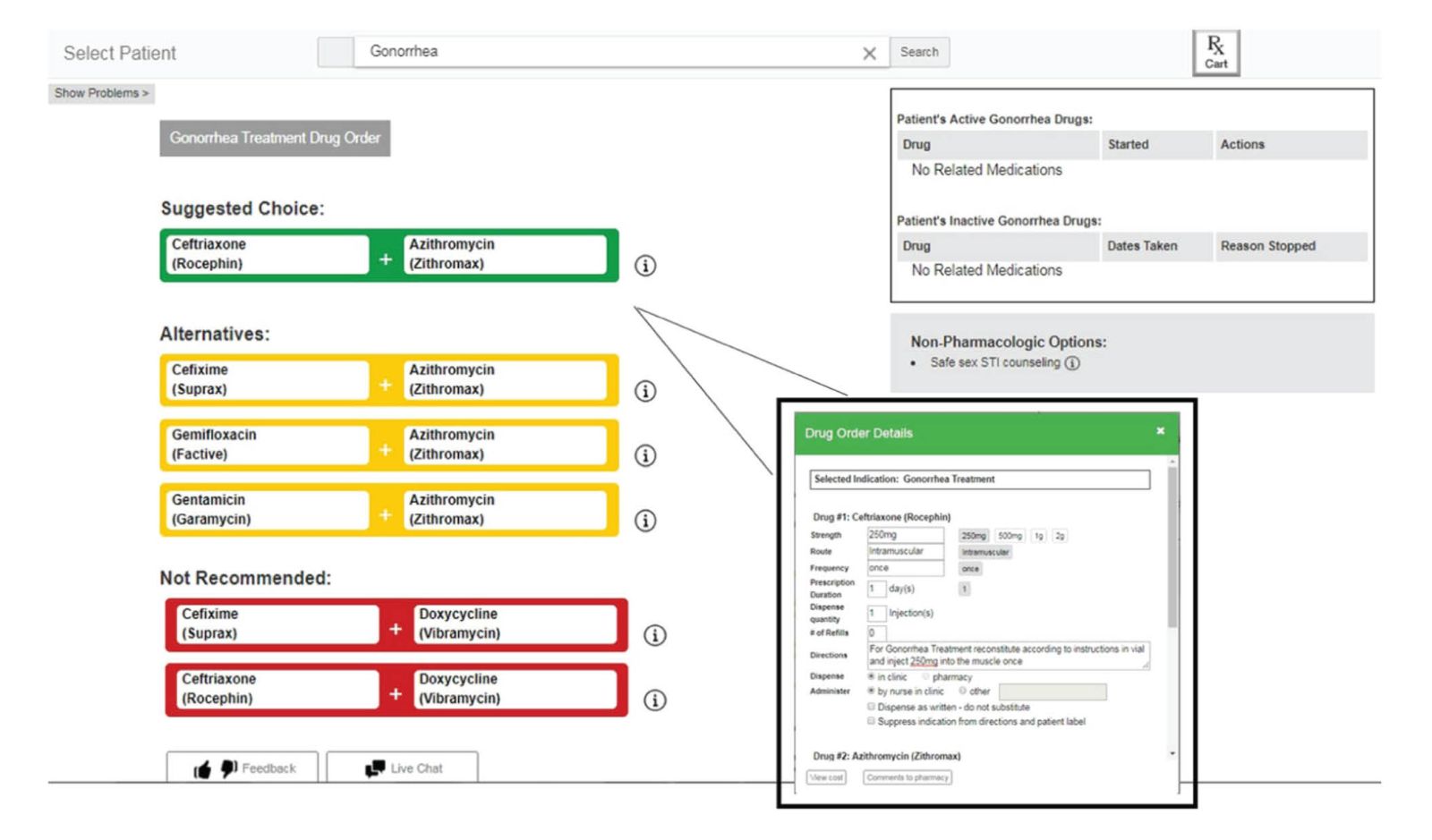
With today’s electronic health records (EHRs), physicians typically begin by entering a drug name rather than the condition they are treating. The prototype instead begins with the indication and suggests recommended treatments, thought to make choosing and ordering the correct drug “faster, easier and safer,” according to a recently published usability study. In the study, the prototype was compared with the order-entry system of two widely used EHRs. Thirty physicians and two physician assistants tested the systems for eight clinical scenarios. The results showed the prototype was faster to use, required fewer clicks, and produced fewer errors. Medication errors, such as drug-allergy indications, occurred in 38 of 128 prescribing sessions using the vendor systems vs. 7 of 128 using the prototype.
With the end of the trial, Schiff says efforts will now focus on working with key players, from the EHR manufacturers and the pharmacy industry, including pharmacy benefit managers and individual druggists as well as patients.
“Physicians need help. The number of drugs is growing. Insurance coverage is kind of chaotic and varies from patient to patient. Rather than relying on memory, personal preference or a drug company recommendation, the computer ought to be helping us with the drugs of choice. That’s the beauty of the system. The challenge is who’s going to populate the drugs of choice.”
Cohen also believes it will require a coordinated effort among clinicians, pharmacists and the major EHR firms. “They’ve invested a tremendous amount of effort in designing the systems that they have out there, and I'm sure they're trying to improve them,” he said. “It's like a 180-degree change for them to start developing a whole new type of software.”
The prescriber enters the indication in the search bar or selects it from a preexisting problem list. Using fictionalized patient data, the prototype suggests drugs of choice with alternatives and drugs that are not recommended. After a drug is selected, an order detail screen appears with most fields prepopulated for dosing and frequency. From JAMA Network Open. 2019;2(3):e191514. doi:10.1001/jamanetworkopen.2019.1514