Q&A: ECRI leaders on a new systems approach to patient safety
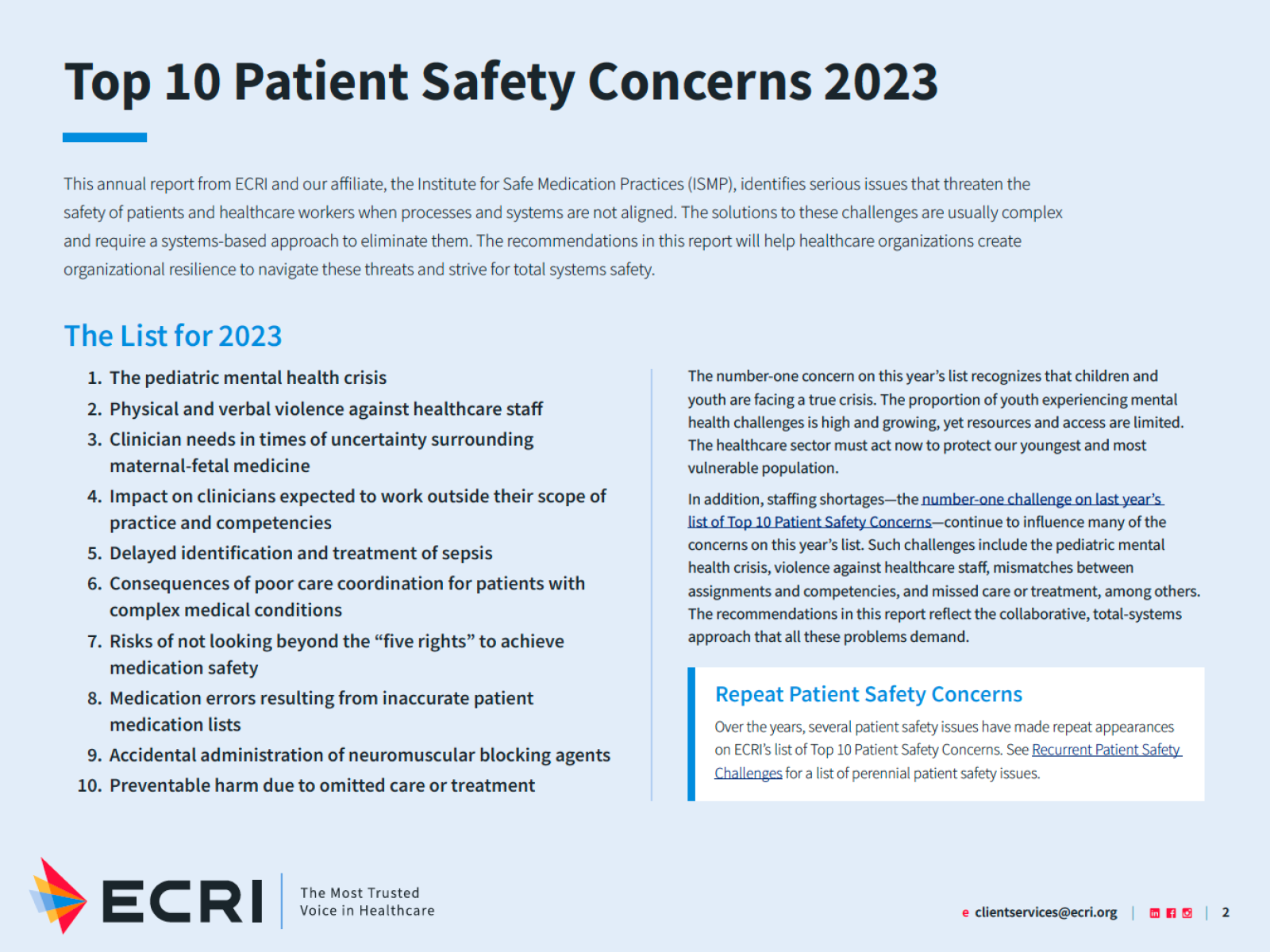
Full list from ECRI
ECRI’s annual top 10 lists — one for health care technology and another for patient safety — highlight urgent hazards and supply analysis and actionable recommendations. The Top 10 Patient Safety Concerns for 2023 includes a new emphasis on system safety. ECRI is an independent non-profit that co-leads one of the U.S. Department of Health and Human Services’ Patient Safety Organizations. Two leaders at ECRI talk with Patient Safety Beat about the list and the current state of patient safety.
Shannon Davila, M.S.N., R.N., is ECRI’s Director of Total Systems Safety. Earlier, Davila served as Director of the Institute for Quality and Patient Safety at the New Jersey Hospital Association and worked in Maine hospitals as a critical care nurse and manager of quality and infection prevention.
President and CEO Marcus Schabacker, M.D., Ph.D., received his medical training in Germany. As part of a humanitarian aid program, he started and led an anesthesia department and intensive care unit at the General Hospital in Mafikeng, South Africa, in the late 1990s. Schabacker then served in leadership roles in the medical device industry before joining ECRI in 2018.

Marcus Schabacker, M.D.

Shannon Davila, R.N.
Patient Safety Beat: The recommendations in your new list of concerns emphasize the need to address gaps in performance with a "total systems approach." Does this involve a different way of thinking about safety challenges?
Shannon Davila: This year, we wanted to strengthen the list’s actionable advice. Everyone at ECRI knows that resources are tight right now at most organizations. People are doing the best they can with what they have. We wanted to focus on ways to help them prioritize and organize their thoughts around these important, complex issues.
ECRI is focused on understanding system design and engineering. We know that to successfully re-engineer health care systems, you have to understand the users of the system — that is, physicians, nurses, patients and families. We have a new team of experts in human factors, which is helping us look at system design and, importantly, also at clinical processes.
Marcus Schabacker: Shannon is our subject matter expert. She has forgotten more about patient safety than I will ever learn. I tend to look at this from a higher level and, as a physician, I start with a level of deep frustration with the current state of patient safety. It’s been more than 20 years since To Err Is Human was published and the Patient Safety and Quality Improvement Act was passed and yet, nearly 100,000 patients die each year from preventable medical errors. I look at ECRI — my own organization — and ask, “What measurable difference have we made in 15 years of being a Patient Safety Organization?” Clearly, we all need to do something different.
When we started to work on this year’s list, the team suggested we add a new element to our thinking and look at high-risk industries that have made tremendous progress in preventing deadly accidents. And while I know we can't fully compare nuclear power or defense or aviation to health care, there's a lot we can learn from them. That's what led us to the total safety system approach.
Health equity is also still a high priority. We know that preventable harm disproportionately affects minority groups, which are not limited to race and ethnicity. The disparity extends to the LGBTQ community, people with disabilities and those who are economically disadvantaged. If we aim for system safety without addressing inequities, we will fail again.
Patient Safety Beat: I think of your organization as a knowledge leader for health technology, including human factors engineering. How does the new team that Shannon mentioned expand on what ECRI has done in the past?
Shannon Davila: What’s new is that we're proactively looking at care processes, looking beyond devices and technology, to understand the path that clinicians are taking, the workflow. We’re looking to expand our work beyond technology, into the practice of care.
What’s new is that we're proactively looking at care processes, looking beyond devices and technology, to understand the path that clinicians are taking, the workflow. We’re looking to expand our work beyond technology, into the practice of care.
Marcus Schabacker: We’ve always had electro-mechanical engineering expertise in-house and some human factors know-how, but it was usually focused on the machine interface. With the help of some external partners, we realized that we’ve been jumping too short. We want to understand the human factor in clinical processes from start to finish. That’s why we brought human factors expertise in-house and consolidated our other experts around looking at processes holistically, not just the human-machine interface.
Patient Safety Beat: Number 3 on the Top 10 list, “Clinician needs in times of uncertainty surrounding maternal-fetal medicine,” is a topic with broad implications. Please share some of what you discussed in developing that idea.
Shannon Davila: When that topic surfaced in our selection process, which takes about three months, we spoke with physicians and practices around the country to gauge how people were feeling. Overwhelmingly, the response was along the lines of, “Yes, please put it on the list. This concerns us every day.” We heard about emergency physicians calling risk managers or the hospital attorney to ask, “When is it OK to do a medical abortion?” In some states, physicians now face trying to determine the potential mortality rate of a pregnant woman who is hemorrhaging. Is it 50%? 90%? This is a patient safety issue. When clinicians are not supported or provided guidance on how to operate within their scope of practice in their state, patient care is compromised. We hope that highlighting this problem will spark conversations at the state level between hospital associations, medical organizations, state departments of health and everyone else to help develop some guidance.
Patient Safety Beat: Dr. Schabacker, given the leadership role anesthesiology has played in the patient safety movement, does your passion for this work come in part from your background as an anesthesiologist?
Marcus Schabacker: As you know, I practiced medicine in South Africa. Toward the end of my practical career, I had a case involving a patient with a post-partum complication and HIV who needed to be intubated and ventilated, and the patient died. The case was investigated and although I was not found guilty in any way, I rack my brain to this day wondering if I could have done something that would have resulted in a different outcome. That was 30 years ago. And so, yes, this is something from my personal experience that is very close and dear to my heart.
I thought perhaps by working in industry, which I did for nearly 20 years, I could improve safety with better product development and in the end, I was disappointed by corporate culture. When I started to wrap up my career and think about what to do with my last 10 years, I discovered ECRI and thought, what a cool organization! We have one aim and one aim only: to make health care better. I can bring my international clinical and industry experiences together and maybe, at the end of my career, finally have an impact on patient safety.
So, that's where that passion comes from. On a human level, having to tell a patient's family that their loved one just died and that it was not necessary — that is the hardest thing to have to do. The trauma, heartbreak and devastation it causes is unnecessary. I just do not understand how we as a profession and a society have arrived at a place where we think it's okay. I don't think it's okay.